Anterior Shoulder Dislocation
The most common cause is traumatic. For example the affected arm is stretched out from the side in a tackle situation when the opponent continues to run past rotating the arm and dislocating the shoulder. It may also occur due to minimal trauma or even a sudden movement without contact. This occurs mostly in individuals with hypermobility of their joints. Other causes include conditions such as epilepsy.
Acute dislocation causes severe pain and loss of function of the shoulder. With a partial dislocation (subluxation) some people will experience a deadness or electric shock sensation down the affected arm. Pain persists until the shoulder dislocation is reduced (put back in joint). Often reduction will require sedation or light anaesthesia to allow sufficient muscle relaxation to occur. The shoulder should be reduced slowly and without undue force.
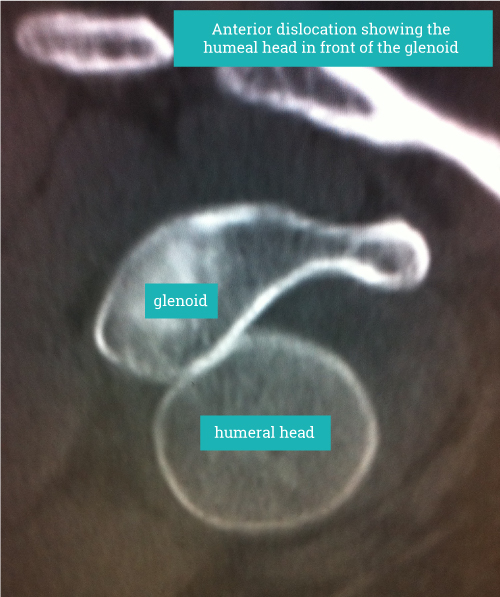
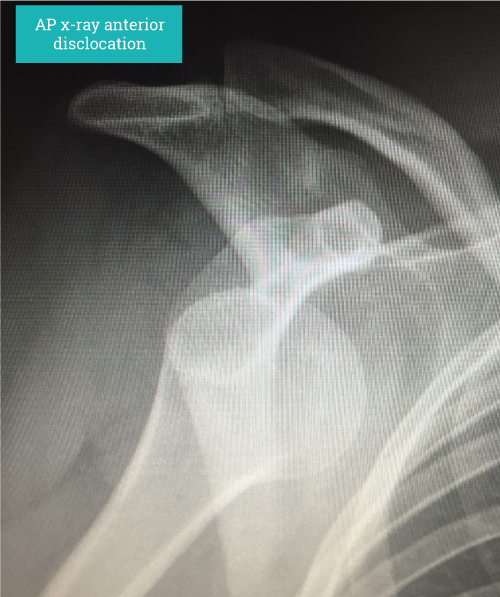
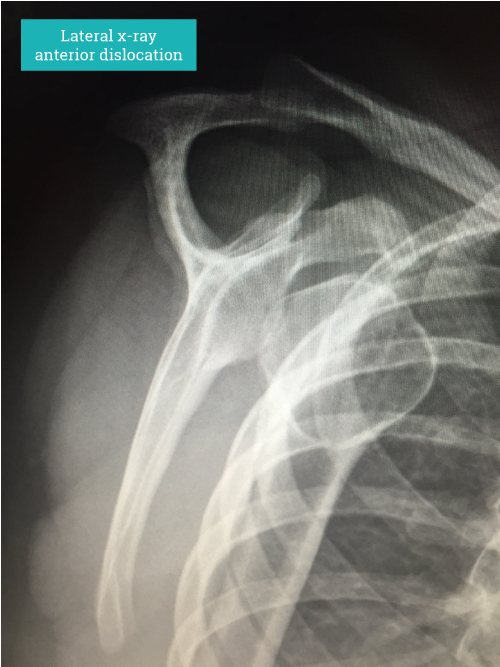
Diagnosis is based on clinical history and signs. Confirmation by an x-ray showing the dislocated shoulder can be helpful. Imaging such as MRI scanning will show the underlying structural problems such as a labral tear (soft tissue Bankart lesion), bony injuries such as glenoid rim fractures (bony Bankart lesion) and impaction fractures on the back of the humeral head (HillSachs lesion) where It has contacted the anterior glenoid during the dislocation. In older persons the risk of damaging the rotator cuff at the time of dislocation is increased and should be actively looked for as rotator cuff tears in these circumstances can be quite substantial.


The axillary nerve should also be assessed clinically. This nerve supplies power to the deltoid muscle and is frequently stretched during a dislocation. Stretching of the nerve results in it not working often for several weeks before spontaneous recovery (most of the time). When the nerve and as a result the deltoid is not working the shoulder will be very weak and elevation of the arm will not be possible without assistance. This returns to normal as the nerve recovers.
Treatment depends on making an assessment of the persons likelihood of recurrence and their wish to proceed surgically or rehabilitate and see what happens.
Higher risk of dislocation is seen in younger athletes in particular those involved in contact sport with the arm outstretched. Other factors increase the chance of dislocation and these include previous dislocation, associated bony injuries such as the bony Bankart and HillSachs lesions described earlier.
Arthoscopic repair( Bankart repair) works well in dislocations without major associated bony injuries. If arthroscopic surgery is planned when there are bony injuries these needed to be addressed at the same time to reduce the risk of redislocation ie arthroscopic remplissage.
When there are significant associated bony injuries we recommend open stabilization using a technique such as a the Latarjet procedure which addresses the bone and soft tissue problems.
“Diagnosis is based on clinical history and signs. Confirmation by an x-ray showing the dislocated shoulder can be helpful.”
Make an appointment
If you wish to make an appointment to discuss your needs further, please get in touch.
Hermitage Medical Clinic
Old Lucan Road
Dublin 20
Call for appointments: 01 6459562
Telephone: +353 1 645 9000
Fax: +353 1 645 9235
Email: info@johnlunn.ie