Rotator Cuff Repair Arthro
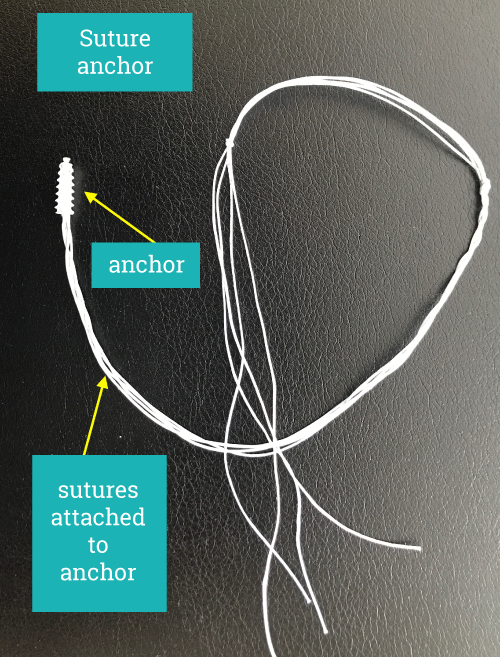
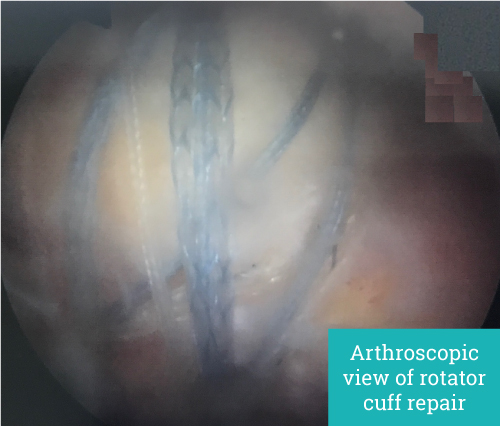
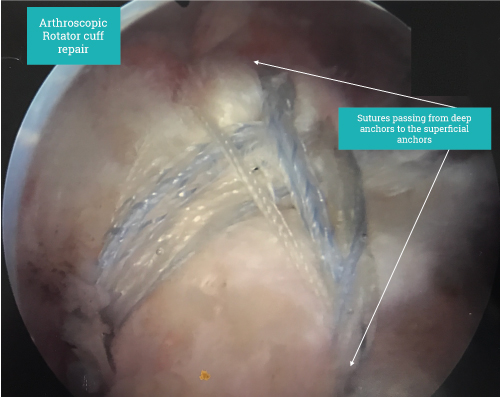
The use of keyhole surgery allows us to see all around the shoulder from different angles and repair all structures without having to compromise due to lack of access. In addition, the deltoid muscle is not split or detached. The rotator cuff is sutured to the bone to allow healing to begin.
Additional procedures such as Subacromial decompression, Acromial-clavicular joint excision, Biceps release or Tenodesis, Suprascapular nerve release and Capsular release are often performed at the same time to address all pain generating problems.
Post-operative course
Following a rotator cuff repair you will have dressings over the small arthroscopic surgical incisions. These remain for 12-14 days after surgery. Drains are not used. Antibiotics will be given in the immediate post-surgical period. Dressings are kept clean and dry. Sutures requiring removal are rarely used. Dissolvable sutures do not need to be removed. Wounds are closed using steristrips which are paper stiches.
The arm is kept in a sling for approximately six weeks. The sling is worn both for comfort and also to remind you not to do any activity that may damage the healing repair. You are encouraged to take the sling off in a safe environment (home) and do simple exercises as per your doctor and physiotherapist. Avoidance of manual work is generally advised until rotator cuff healing has occurred; in general, this is around 12 weeks after surgery.
Return to driving is around 6-8 weeks once the patient is out of the sling and feels safe to drive. Pain requiring regular analgesia for the first 2-3 weeks is not uncommon. Pain relief is taken as needed.
Rehabilitation
This is done under the supervision of your surgeon and physiotherapist. Rotator cuff tears are not all the same and may require different rehabilitation programmes. The initial period in the sling limits rehabilitation with goal being to maintain comfortable passive range of movement. Once the sling is removed progress often feels slow as you try to regain normal range of movement. Strengthening is not generally started until a minimum of three months. Prolonged repetitive overhead activity should be avoided
Risks and Complications are rare and most patients have good outcomes from surgery.
Pain from the neck or sources other than the shoulder will not be improved by surgery on the shoulder, for example numbness or pain in the hand, wrist, elbow or neck is typically not caused by a problem in the shoulder.
Any surgery on the shoulder risks the development of post-operative inflammation. This causes the shoulder to become stiff and painful for several months before resolving spontaneously. Most shoulders after rotator cuff repair will be stiff but this resolves slowly as healing progresses.
Other complications are rare. Infection occurs in 1/500 individuals. This is a serious complication which may present late and be difficult to diagnose. Infection requires further surgery and a prolonged course of antibiotics. After an infection your shoulder may be permanently damaged.
Damage to nerves or blood vessels around the shoulder is rare but may result in permanent weakness/ loss of sensation affecting the entire arm.
Complications related to anaesthesia range from a sore throat to cardiac or respiratory problems. Any pre-existing medical problems may flare up after an anaesthetic and surgery. Ideally all medical conditions should be as optimized as a much as possible before surgery. This may involve seeing a cardiologist or other medical physician prior to surgery.
Blood thinning drugs should be stopped prior to surgery with the exception of aspirin which should be continued.
“Rotator cuff tears are not all the same and may require different rehabilitation programmes.”
Make an appointment
If you wish to make an appointment to discuss your needs further, please get in touch.
Hermitage Medical Clinic
Old Lucan Road
Dublin 20
Call for appointments: 01 6459562
Telephone: +353 1 645 9000
Fax: +353 1 645 9235
Email: info@johnlunn.ie